The Roadmap
A patient registry project usually starts out with the goal of obtaining new insights from clinical data. Data that were not previously available in a structured format, and which therefore could not be analyzed, need to be collected.
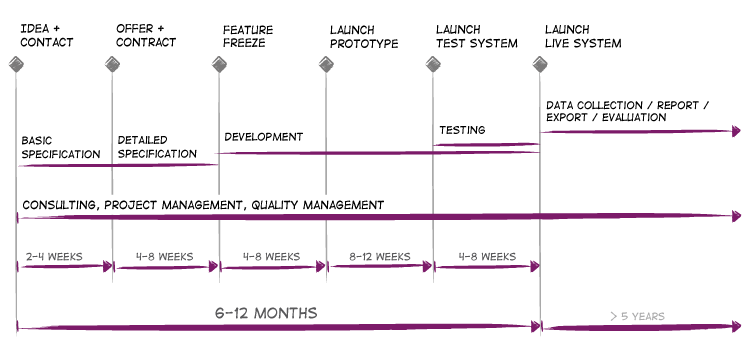
As an experienced partner, we accompany patient registry projects from their inception and subsequent development until a registry has come to the end of its service life. An interdisciplinary project group works on the design and implementation for a period of between six and twelve months. Ideally, patient registries then run for a period of at least five years.
Contact us

It is becoming increasingly common for the authorities to require the documentation of particular treatments even after having been approved – i.e. post-marketing surveillance (PMS). More often than not, however, the request comes from the scientific community or directly from a project sponsor. Sometimes the initiative for a new patient registry even comes from us.
Help getting started
Would you like to initiate a clinical patient registry, but there are still so many unanswered questions and you are not quite sure exactly how such a project could unfold?
Contact us – we will help you to get the project up and running successfully. We have over 15 years of experience with projects in the healthcare sector and are familiar with the demands of all parties involved in such projects: the pharmaceutical industry, scientists, patients and, increasingly, the authorities.
Length: Very short
An e-mail or a telephone call is all that is needed:
Martin Verdino, VERDINO
Weyringergasse 3, 1040 Vienna, Austria
+43 1 227 60 38
Project specifications and getting an offer
We are able to deal some questions straightaway by e-mail or telephone. If it is possible to arrange a face-to-face meeting, we can then discuss the project objectives and the scope of the project in direct dialogue. To do this, we are more than happy to come you – however many of our customers and project partners prefer to come to our conveniently located offices in the center of Vienna.
The first step is to agree on the requirements and the framework conditions in as much detail as possible. Doing so enables us to estimate the scope of the project, the starting situation, the complexity and, not least, the approximate timetable.
Estimating costs and getting an offer
Obtaining an accurate estimate of the framework conditions and scope of our consultancy services is the only way to be able to estimate costs properly. After receiving your feedback, we make a binding offer for both initial and ongoing costs. The scope of the offer can also be widened in the future and additional services offered.
Length: Short
Just a few e-mails and telephone calls to discuss can be enough here. A face-to-face meeting can speed up this step further.
Information architecture
Once the offer has been accepted, work begins on designing the registry, putting together the necessary data fields and associated structures.
Option 1: Database or detailed data structure already exists
If a database already exists, the data structure can be used as the basis for the new registry database. The details of any changes required must be agreed on – normally this does not require too much time.
Option 2: No preliminary work available
If there is just an idea but no exact and structured list of the necessary data fields, we help the initiators to do this groundwork. Medical experts bring their specialized knowledge and we help to structure the information with tried-and-tested tools. At the end of this process, the basis for the new registry database has been created.
During this project phase, we recommend analyzing a number of current patient files in detail – particularly if a detailed data structure does not yet exist. The data available here can be used as the basis for the future data structure, helping to avoid time-consuming changes to the data structure at a later point in time.
Defining the features
While the data structure is being created, the required features and data field dependencies are defined. To ensure that, in an interdisciplinary project team, we all speak the same language and come to a solution that really works in practice as efficiently as possible, we make use of existing solutions and prototypes. In many cases, it is then just a case of identifying the extent to which we need to depart from the standard solution.
The result
The completed information architecture outlines the content (text, images, forms, lists, etc.) and functions (calculations, graphical and statistical analyses, data exports) that will be used in the future registry.
Length: Two weeks or more
The details are agreed via e-mail and telephone. Face-to-face meetings can speed up this step considerably.
Prototype

Based on the content and features defined, a prototype is developed that is a 1:1 imitation of the future registry but which is not yet functionally linked to database. You can navigate around the registry and find out how the interface of the future registry solution actually looks and feels. Data can also be entered into the fields, but these are not yet stored in the database.
The prototype helps us to see quickly if any data fields are missing, if any necessary functions and calculations have not been included or if there are any occasional details that have not quite been implemented properly. The web-based prototype can also be evaluated once again by independent experts – providing additional quality assurance.
Length: Four weeks or more
During this phase, only a few details need to be clarified by e-mail or by telephone. The finished prototype should be presented to the working group face-to-face at least once.
Implementing and testing

The final, approved prototype forms the basis for the application and the database and which is to be modified to accommodate individual requirements. Every patient registry contains different data fields with varying structures and functions, even if the basic structure is very similar.
Once these modifications have been made, the patient registry solution is handed over to the working group for testing. Unlike the prototype, the test system is fully functional. During the test phase, real data can and should be used to make sure that the system functions properly. Should there be any isolated errors, these can be quickly resolved.
Length: Twelve weeks or more
During this phase, only a few details need to be clarified by e-mail or by telephone. The finished patient registry should be presented to the working group face-to-face at least once.
Launch

Once the test system has been given final approval, the system goes live. From this point on, all participating centers and physician accounts can be created. Data collection can also start immediately.
Length: Very short
Acceptance of the test system in writing is all that is needed. The live system can then be switched on.
Operations and further development
Operations and ongoing support
Once live, the registry runs on highly secure servers with a fail-safe design and which make it possible to input and analyses data at any time of the day or night. Data entered into the registry database are automatically stored and regularly archived in state-of-the-art back-up systems. At the same time, multiple security systems (firewalls, intrusion detection systems) provide the highest level of security for your valuable data.
Our IT specialists ensure that all systems are updated on a regular basis during operation so that your registry always has the latest security and IT technology.
Further development
After launching the first phase, additional modules are developed and implemented step by step in almost every project. It is often the case that, during operation, modifications are made to the live system after successful testing.
Associated communication
Numerous projects are also accompanied by associated communication strategies such as registry brochures, information websites for interested members of the public or a regular meeting for registry participants. As a communications agency, we are also able to provide a great deal of experience and expertise here.
Things to remember
Aside from the software, which is critical for collecting data, a number of supporting organizational measures need to be considered.
Along with a working group, which primarily concentrates on initial development, it is advisable to set up a board (board of directors, scientific advisory board) and an administration team with a registry coordinator for the operations, as well as perhaps study nurses.
In addition, contracts should be drawn up between the participating centers (which include the exact definition of publication rights) and patient declarations of consent prepared.
Finally, related communication activities and regular registry meetings should be planned.